Understanding Parietal Lobe Seizures: Meet Amelia
Parietal lobe seizures are focal seizures that begin in the parietal lobe, the brain region that helps you feel your body, locate yourself in space, and make sense of touch, temperature, movement, and body position. Because many symptoms are internal and difficult to articulate, these seizures are often misunderstood or misdiagnosed. In this post, the story of Amelia will be woven throughout to illustrate how these seizures can unfold in real life, bringing clinical features into relatable context. Through her experience, you will learn what parietal lobe seizures can feel like, why they can be challenging to confirm on routine tests, what clinicians look for during evaluation, and how treatment is approached.
Dr. Clotilda Chinyanya
2/2/20269 min read


Amelia’s story
Amelia was halfway through her morning routine when the world did something that did not fit into any normal category.
She was standing at the bathroom sink, brushing her teeth, when her left hand suddenly felt wrong. Not painful at first. Just unfamiliar. It was still her hand, still attached, still visible, but it did not feel like it belonged to her in the usual way. A strange buzzing traveled from the tips of her fingers into her palm, as if her skin had become a low electric field.
She paused, toothbrush still in her right hand. The buzzing sharpened into pins and needles, then moved, climbing her wrist like a ripple. She tried to shake it off, the way you would after sleeping on your arm, but the sensation did not behave like numbness. It had direction. It marched upward.
Then came the second layer of strangeness. Her arm felt longer than it should be, as if it stretched past the sink, past the mirror, past the room. She looked down and saw the same arm she always had. Yet her brain insisted it was changing shape. She swallowed hard and stared at her reflection, trying to talk herself out of panic.
The buzzing reached her forearm, and for a moment, she felt as if her elbow twisted in a way it did not. Her posture stayed still, but inside, something signaled movement that never happened. She felt a brief vertigo, the room tilting like a boat, and she grabbed the counter.
It lasted maybe twenty seconds, maybe thirty. Time itself felt elastic. When the sensation released, it left her with an aftertaste of fear and confusion. She rinsed her mouth, hands trembling, and told herself it was stress. Lack of sleep. Too much coffee.
But it happened again two days later while she was walking to her car. This time it started with a crawling feeling in her left foot, like invisible ants under the skin. The sensation moved upward, and as it climbed, her body tensed. She stayed aware, fully awake, watching the sidewalk, counting her breaths. She made it into the car and sat there, palms open, waiting for the world to return to its normal rules.
After the third episode, Amelia stopped calling it stress. She started writing notes in her phone. Where was the sensation. How it moved. Whether she felt dizzy. Whether her body felt distorted. Whether she could speak. She noticed something else too. The episodes sometimes followed touch or movement. Once, after she rubbed lotion into her left ankle, the tingling began almost immediately.
At her appointment, the neurologist listened carefully, not just to the symptoms but to the pattern. Amelia described the tingling that marched along her limb, the brief sense that her arm changed size, the strange internal motion in a still body, and the moments of vertigo. The neurologist explained that the parietal lobe is a sensory integration hub, and when a seizure starts there, it can produce vivid sensory and body perception changes, sometimes with awareness fully preserved (1,2).
Her first routine EEG did not give a clear answer. That did not surprise the neurologist. Parietal lobe seizures can be difficult to localize on scalp EEG, and the seizure activity may be subtle or may spread quickly to other regions (1,3). The plan was to keep going. More detailed imaging. Longer monitoring. A careful search for an underlying cause.
For the first time in weeks, Amelia felt something soften inside her. Not because she wanted a diagnosis, but because she needed her experience to make sense. She needed a map.
What are parietal lobe seizures?
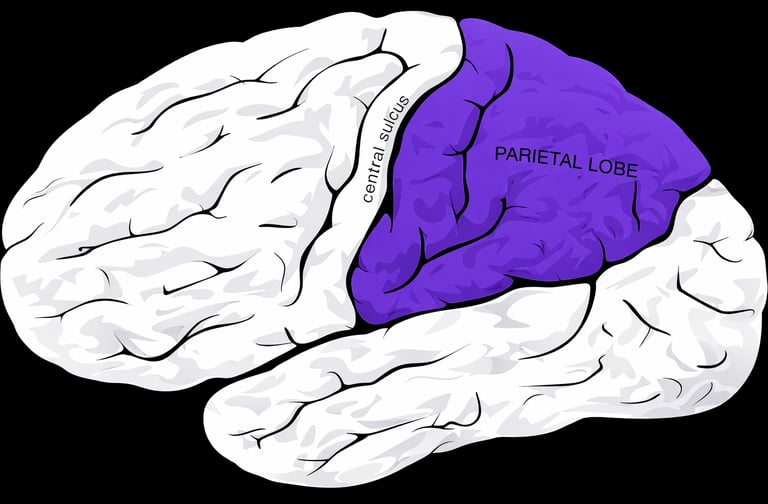
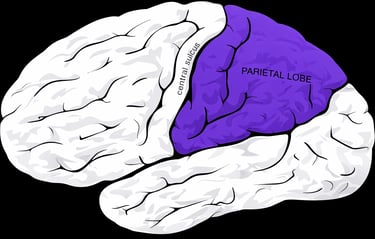
The parietal lobe is located near the top and back portion of the brain, sitting behind the frontal lobe and above the temporal lobe, extending toward the occipital lobe at the rear. It lies just behind the central sulcus, where the primary sensory cortex in the postcentral gyrus processes incoming sensory information from the body. See image below:
The parietal lobe is primarily responsible for interpreting touch, pain, temperature, and proprioception, which is your sense of body position and movement in space. It helps you recognize where your limbs are without looking, judge distance, navigate your environment, understand spatial relationships, and coordinate hand eye movements. In the dominant hemisphere, it also contributes to reading, writing, calculation, and aspects of language comprehension. In short, the parietal lobe helps you feel your body accurately and orient yourself within the world around you (1,2).
When a seizure begins in this region, symptoms often present as sensations and perceptions rather than dramatic outward movements. That is why many people struggle to describe them, and why clinicians often rely on detailed history, patterns, and careful classification.
Core symptoms
Parietal lobe seizures commonly involve positive (excessive) sensory symptoms, negative (reduced) sensory symptoms, or both (1,2).
Common experiences include:
· Tingling, numbness, pins and needles, prickling, crawling, or an electric shock feeling in one body area, often on the side opposite the seizure onset (1).
· Painful sensations or abnormal temperature perception, such as burning or cold (1,2).
· Vertigo or a sudden sensation of spinning or falling (1,2).
· Body image distortions, such as feeling a limb is enlarged, shrunken, missing, elongated, shortened, or moving when it is still (1,2).
· Visual illusions near the parieto occipital junction, such as micropsia or macropsia, where objects appear smaller or larger than they are (1).
· Language related difficulties when dominant hemisphere regions are involved, including problems with reading, writing, and calculation (1,2).
· Mouth and tongue sensorimotor symptoms, speech difficulty, drooling, and sometimes autonomic sensations or emotional shifts, particularly when networks involving the operculum and connected regions are engaged (1).
A key reality is that parietal lobe seizures often spread quickly into other lobes. When that happens, the most visible symptoms can reflect where the seizure goes, not where it started (1,2). This is one reason parietal lobe epilepsy has been called a great imitator.
Subtypes based on where seizures start in the parietal region
Clinicians sometimes describe patterns based on parietal subregions. These patterns help make the symptoms more predictable and interpretable (1).
· Primary sensory area: Often begins with a focal sensory seizure, commonly tingling or numbness on the opposite side. The sensation can travel in a sequence across the body map, called a Jacksonian march. Motor activity can follow if the seizure spreads into motor networks (1).
· Non dominant parietal cortex: Distorted sense of one’s own body may be the main feature. People may feel floating, twisting, altered posture, or body part size distortions such as enlargement, shrinking, absence, or unusual length changes. Distal areas and the tongue are often described (1).
· Secondary sensory area: May produce cognitive sensations followed by a feeling of inability to move, sometimes spreading sequentially, sometimes followed by clonic jerking (1).
· Parieto-occipital junction: Often linked to visual illusions such as objects appearing larger or smaller than they are. Some people may experience uncontrollable eye movements. Awareness is retained (1).
· Paracentral lobule: Can involve sexual sensations and occasionally sexualized behavior when networks in this area are engaged (1).
· Dominant parieto-temporal region: May produce language and calculation difficulties, including trouble reading, writing, and arithmetic (1).
· Fronto-parietal operculum: May cause mouth and tongue symptoms, speech difficulty, drooling, and may include autonomic, emotional, or gustatory features due to network connections (1).
Why parietal lobe seizures are often misdiagnosed
Many symptoms are subjective and can resemble migraine aura, transient neurologic events, anxiety or panic, functional neurologic episodes, or psychiatric symptoms (1,4). The unusual nature of body distortions and perceptual changes can be especially confusing for patients and clinicians alike.
In addition, routine tests may not easily capture the seizure onset zone. Scalp EEG may be non-localizing, and even ictal scalp EEG can be unhelpful, sometimes appearing normal in a large proportion of events (2,3). That does not mean the events are not epileptic. It means the signal may be deep, subtle, or rapidly spreading.
Diagnosis and evaluation
Diagnosis rests on four pillars: history, exam, EEG strategy, and imaging.
· History: A precise description of the aura matters. Where it starts, how it spreads, whether awareness is retained, whether there are triggers such as touch or movement, and whether the episodes are stereotyped is often decisive (1,2,5).
· EEG: Routine EEG can miss the focus. Some individuals show posterior or central parietal abnormalities, but others have normal recordings, especially when the onset is mesial or when spread dominates the scalp pattern (3). Longer video EEG monitoring, sleep recordings, and targeted protocols can improve yield.
· Imaging: Structural causes are important to evaluate, including focal cortical dysplasia, vascular lesions, tumors, trauma related changes, and prior infections or stroke (2,5). Subtle lesions can be missed on standard reads and may require high resolution protocols, postprocessing, or multimodal imaging.
Triggers and a notable pattern: Proprioceptive induced seizures
A small subset of people experience seizures triggered by proprioceptive stimuli, such as rubbing a body part, stepping on uneven ground, or specific limb movements. These can be mistaken for movement disorders because the trigger is movement and the outward expression can look like dystonia or abnormal posturing (5).
One well described clinical lesson is that careful attention to the presence of sensory aura, lateralized symptoms, preserved awareness, and poor long term response to a movement disorder framework can point back toward parietal lobe epilepsy (5).
Treatment and living with parietal lobe seizures
Treatment depends on cause, seizure burden, and how the seizures respond.
· Anti-seizure medications: Many people are treated with anti-seizure medications, sometimes called anti epilepsy drugs. The goal is seizure freedom with minimal side effects. Medication choice is individualized based on seizure type, comorbidities, age, pregnancy considerations, and interactions. In some structural epilepsies, an initial response can occur, but drug refractoriness may develop over time (5).
· Addressing the underlying cause: If imaging reveals a structural lesion that is driving seizures, management may include lesion directed strategies.
· Surgery: When seizures continue despite appropriate trials of anti-seizure medications, referral to an epilepsy center is important. Surgical outcomes can be favorable in selected patients, especially when a lesion is identified and the seizure onset zone can be mapped while protecting eloquent cortex (2,5).
· Safety and self-management: Because parietal seizures can include vertigo, body schema distortion, and sudden sensory changes, practical precautions matter. Consider situational risk. For example, bathing alone, climbing ladders, or driving without clearance can be hazardous. Keeping a seizure diary, capturing triggers, and asking witnesses to describe observed behaviors can help the care team refine diagnosis and treatment (1,4).
How to describe episodes clearly
If you think you or a loved one might be having parietal lobe seizures, use structured language.
· Onset: Where did it start in the body or perception. Fingers, foot, tongue, face, visual field, sense of posture.
· Spread: Did it move. In what direction. Over what time. A marching pattern is important to note (1).
· Awareness: Could you understand others and remember the episode.
· Associated features: Vertigo, visual distortions, inability to move, speech difficulty, fear, autonomic sensations, or post episode headache or fatigue (1,2).
· Triggers: Touch, rubbing, movement, sleep deprivation, stress, or sensory stimulation can be relevant (3,5).
Amelia’s notes did not just record symptoms. They built a clinical story. That is often how parietal lobe seizures become visible, not through a single dramatic test, but through a pattern that repeats with the same signature.
Prognosis
Parietal lobe epilepsy is not classified as a self limited childhood epilepsy syndrome and is often related to structural or focal causes, meaning long term management may be required. The long-term outlook depends largely on the underlying cause and how well the seizures respond to treatment. If no structural abnormality is found and seizures respond well to anti-seizure medications, many people can achieve good control and live full, stable lives. However, when a structural lesion such as focal cortical dysplasia is present, seizures are more likely to become drug resistant, and evaluation at a specialized epilepsy center may be needed. In carefully selected cases, surgery can offer significant seizure reduction or even seizure freedom.
In Amelia’s case, no structural lesion was identified on imaging, and her seizures responded to anti seizure medication. She did not require surgery. With treatment, monitoring, and lifestyle adjustments, her episodes became controlled, allowing her to regain confidence in her daily routines while continuing regular neurologic follow up.
Your Symptoms Matter
If your experiences feel unreal, confusing, or difficult to describe, do not dismiss them. Unusual sensory or body perceptions can still be neurological. Pay attention to patterns, write down exactly what happens, when it starts, how it spreads, how long it lasts, and whether you remain aware. Then bring that detailed record to a medical professional. A clear, consistent history can make the difference between being misunderstood and getting the right diagnosis and treatment.
Reference list:
1. Parietal Lobe Seizure Clinical Overview
International League Against Epilepsy EpilepsyDiagnosis.org
https://www.epilepsydiagnosis.org/seizure/parietal-overview.html
2. Salanova V. Parietal lobe epilepsy. Journal of Clinical Neurophysiology. 2012
PubMed link
https://pubmed.ncbi.nlm.nih.gov/23027096/
3. Parietal Lobe Seizure EEG and Diagnostic Features
International League Against Epilepsy EpilepsyDiagnosis.org
https://www.epilepsydiagnosis.org/seizure/parietal-eeg.html
4. Parietal Lobe Seizure Differential Diagnosis
International League Against Epilepsy EpilepsyDiagnosis.org
https://www.epilepsydiagnosis.org/seizure/parietal-differential.html
5. Zheng Y, Ming WJ, Zheng Z, et al. Pearls & Oy-sters: Parietal Lobe Epilepsy in Disguise Motor Attacks Induced by Proprioceptive Triggers. Neurology. 2022;98:509 to 513
https://doi.org/10.1212/WNL.0000000000200050
6. Duncan JS. Occipital and parietal lobe epilepsies. Epilepsy Society Chapter Review
https://epilepsysociety.org.uk/occipital-and-parietal-lobe-epilepsies
7. Frontiers in Neurology. Parietal Lobe Epilepsy Review Article
https://www.frontiersin.org/articles/10.3389/fneur.2022.XXXXX
8. Epilepsy Society. Focal Seizures Information Page
https://epilepsysociety.org.uk/about-epilepsy/seizures/focal-seizures
Choose Knowledge: